How Do You Know if You Have a Inguinal Hernia
Hernias are a mutual surgical pathology that is poorly understood past medical students and junior trainees. Getting to grips with the underlying beefcake will hopefully provide you with the framework to be able to understand, diagnose and capeesh the principles of their management.
You may besides be interested in our guide to hernia examination.
What is a hernia?
The often recited surgical definition of a hernia is 'the protrusion of a viscus into an abnormal space'. In elementary terms, a hernia describes a construction that passes through a space or defect, into an abnormal location.
This commodity volition hopefully provide an overview of the more common abdominal hernias and a brief description of how they can be managed. Before we dive into the different types, I wanted to unpick some of the mutual terms used in relation to hernias (east.thou. "56 year-erstwhile-male with an irreducible inguinal hernia").
- Reducible: when the contents of the hernia tin can be manipulated back into their original position through the defect from which they sally
- Incarcerated hernia (irreducible): the hernia is compressed past the defect causing it to exist irreducible (i.east. unable to be pushed back into its original position)
- Obstructed hernia: refers mainly to hernias containing bowel, where the contents of the hernia are compressed to the extent that the bowel lumen is no longer patent and causes bowel obstacle
- Strangulated hernia: the compression around the hernia prevents blood flow into the hernial contents causing ischaemia of the tissues and associated hurting
The most mutual blazon of abdominal hernia is an inguinal hernia, which typically presents with a lump in the groin. I think it is best to first look at the basic anatomy of the inguinal canal to assist the understanding of the clinical findings and and so move on to the principles of management.
You might also be interested in our surgical flashcard collection which contains over 500 flashcards that comprehend key surgical topics.
Beefcake of the inguinal canal
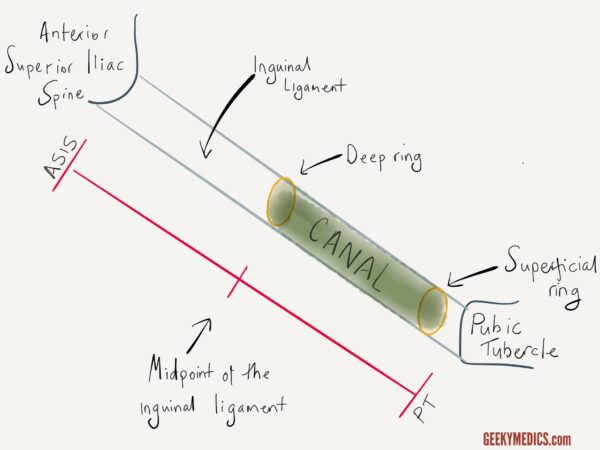
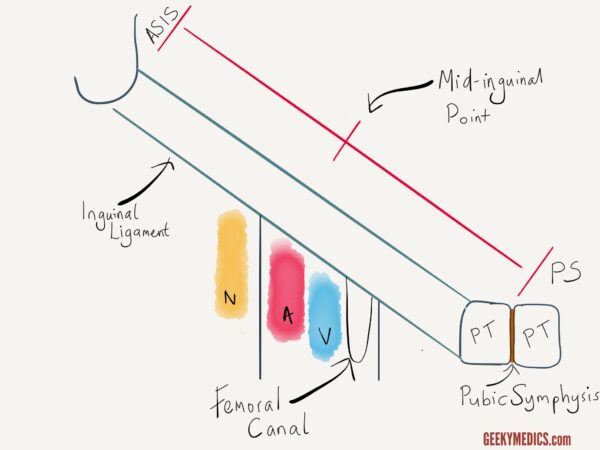
The inguinal ligament runs between the anterior superior iliac spine (ASIS) and the pubic tubercle (PT). Inside this ligament runs a tube-like structure known as the inguinal canal. The function of this canal is to provide a passageway for abdominal contents to exit the abdomen. To be more specific, in males this is the spermatic string (to facilitate ejaculation), and in females the round ligament. In both sexes, the canal also carries a sensory nervus known as the ilioinguinal nerve. The tube has an entry point from the abdominal cavity into the culvert (deep inguinal band) and an leave point (superficial inguinal ring) as it leaves the canal. The location of these two points is clinically important and is also a common test question. The deep inguinal band is located just higher up the mid-signal of the inguinal ligament. The superficial ring lies just to a higher place and lateral to the pubic tubercle (see illustration beneath).
Deep vs superficial inguinal ring
Deep inguinal ring: but above the midpoint of the inguinal ligament
Superficial inguinal ring: only higher up and lateral to the pubic tubercle
Direct vs indirect inguinal hernias
An inguinal hernia is a protrusion of abdominal contents that ultimately emerges from the superficial inguinal band. In that location are 2 main ways in which inguinal hernias can arise, which are discussed below.
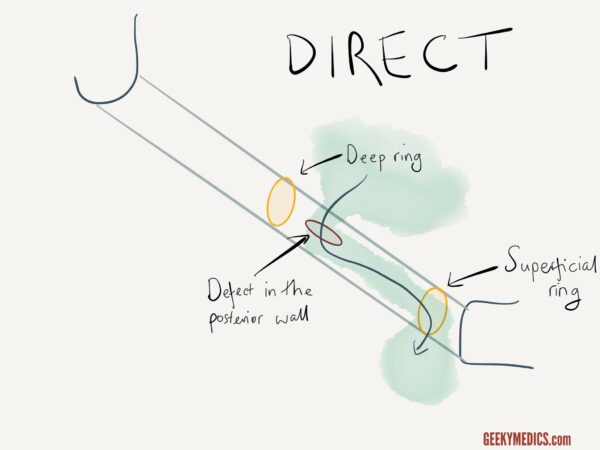
Straight inguinal hernia
A straight inguinal hernia is caused by a weakness in the posterior wall of the inguinal culvert. The abdominal contents (unremarkably just fat tissue, sometimes with bowel) are forced through this defect and enter the inguinal canal. This means that the contents emerge in the culvert medial to the deep ring (as shown).
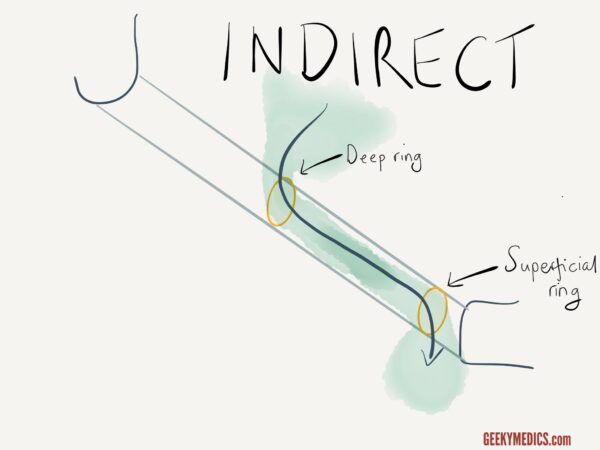
Indirect inguinal hernia
An indirect inguinal hernia, still, does not pierce the posterior wall. The intestinal contents laissez passer through the deep inguinal ring, passing through the inguinal canal and exiting via the superficial ring.
Differences betwixt indirect and direct inguinal hernias
Both types of hernias can exit via the superficial ring and emerge within the scrotum, still, information technology is more common for indirect inguinal hernias to do this every bit the path through both anatomical inguinal rings, rather than a musculus defect, has less resistance.
An appreciation of the anatomical differences can assistance to distinguish between the two using clinical exam. The principle of this is that if you can place your finger over the deep inguinal ring (merely in a higher place the mid-point of the inguinal ligament), and then y'all can command an indirect inguinal hernia which has been reduced. If when yous press the deep band, the hernia however protrudes, then the hernia is emerging via a defect in the posterior wall medial to this point and is, therefore, a direct hernia. It is useful to sympathise this clinical test as it helps call back the divergence between the 2. The clinical awarding of this kind of assessment, nevertheless, is express as it is non very reliable and doesn't alter direction.
What causes an inguinal hernia?
The easiest way to think virtually the causes of inguinal hernias is to remember of:
- Increased intra-intestinal pressure level
- Weakness of the abdominal muscles
The causes are, therefore, every bit follows:
- Chronic coughing
- Constipation
- Heavy lifting
- Advanced age
- Obesity
How do hernias present?
Virtually commonly patients will present to their GP, with a painless swelling in the groin that develops over time.
The swelling is oft otherwise asymptomatic and may come and get.
Alternatively, the swelling may have emerged all of a sudden after heavy lifting, for example.
Symptomatic hernias
Hernias tin can get symptomatic, presenting with clinical features such as:
- Pain: particularly when coughing or stooping
- Alter in bowel habit
- Constipation
- Burning sensation in the groin
- Scrotal swelling (in males)
The majority of inguinal hernias can be accurately identified with a clinical examination. Where at that place is diagnostic dubiousness an ultrasound scan of the groin can assist differentiate between other possible causes such equally enlarged lymph nodes, fat lumps, or vascular pathology.
So when and why practice we ready them?
It is a common-sense approach with regards to the management of inguinal hernias. If the lump is small, not increasing in size and is asymptomatic the patient may wish to go out it alone. If withal the hernia is causing pain or altering bowel habit then surgical management may be required. If the hernial contents become strangulated or obstructed this represents a surgical emergency and urgent operative fixation is required.
Both straight and indirect inguinal hernias are repaired in the same way. The main conclusion to be fabricated is whether to fix the hernia via an open or a laparoscopic technique.
Open inguinal hernia repair
An open technique explores the inguinal culvert, identifies the important structures within it (which need to be advisedly protected), reduces the hernial contents back into the abdominal cavity and places a mesh that strengthens the posterior wall to prevent farther herniation. Information technology is a simple functioning with excellent results and can exist done with either full general or local anaesthetic.
Laparoscopic inguinal hernia repair
Laparoscopic inguinal hernia repair is likewise an splendid operation in experienced easily. It has the added benefit of less mail-operative pain and quicker recovery, particularly if bilateral hernia repair is performed. The basic steps of the performance involve visualising the defect from within the abdominal cavity, reducing or pulling back the contents of the hernia, and repairing the defect from within the abdomen.
Femoral hernias
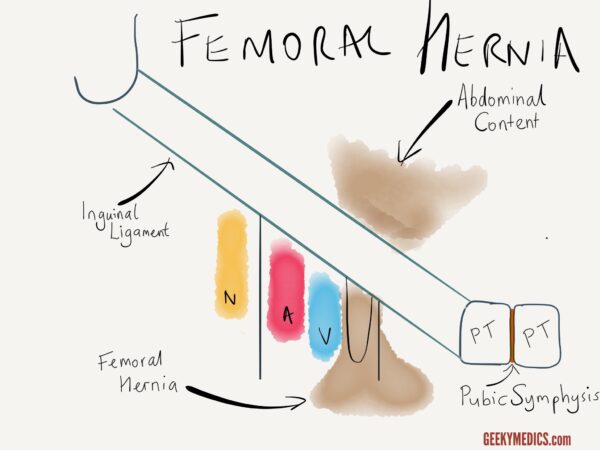
Passing beneath the inguinal ligament are some important structures travelling to the upper leg. Most notably this includes the femoral artery, the femoral vein and the femoral nerve. The order in which these structures lie is easily remembered past the 'NAVY VAN' mnemonic. With the 'Y' signifying the creases of the groin, it illustrates how from lateral to medial the structures lie (nervus, artery, vein).
The femoral artery and vein are enclosed within a sheath (see diagram below). Lying medial to the femoral vein is a space known as the femoral canal. The function of this infinite is to allow expansion of the femoral vein in order to increase venous return. In health, the femoral canal contains just a small amount of fat tissue and a lymph node (known every bit the lymph node of Cloquet).
This space, particularly in elderly women, can be a defect through which abdominal contents can protrude. Information technology is of import to annotation that this space is quite tight, and it is bordered medially by the sharp edge of the lacunar ligament. Therefore, femoral hernias are at high risk of strangulation and obstacle.

How Do You Know if You Have a Inguinal Hernia
Source: https://geekymedics.com/hernias-explained/
0 Response to "How Do You Know if You Have a Inguinal Hernia"
Post a Comment